

What Is The Composition Of Our Skin
Nurses need to understand the skin and its functions to identify and manage peel problems. This article, the first in a 2-function series, looks at the skin's structure and cardinal functions. This article comes with a self-assessment enabling you lot to test your noesis afterwards reading it
Abstract
Skin diseases touch on 20-33% of the population at whatsoever ane time, and around 54% of the Britain population will experience a skin condition in a given year. Nurses discover the skin of their patients daily and it is important they sympathize the skin so they can recognise bug when they arise. This commodity, the get-go in a two-function series on the skin, looks at its structure and office.
Citation: Lawton S (2019) Skin i: the structure and functions of the skin. Nursing Times [online]; 115, 12, thirty-33.
Writer: Sandra Lawton, Queen's Nurse and nurse consultant and clinical lead dermatology, The Rotherham NHS Foundation Trust.
- This article has been double-blind peer reviewed
- Scroll downwardly to read the article or download a print-friendly PDF here (if the PDF fails to fully download please try once again using a different browser)
- Assess your cognition and gain CPD evidence by taking the Nursing Times Self-assessment test
- Read part 2 of this series here
Introduction
Skin diseases affect xx-33% of the UK population at any one time (All Parliamentary Grouping on Skin, 1997) and surveys suggest around 54% of the Britain population will experience a peel status in a given year (Schofield et al, 2009). Nurses will discover the peel daily while caring for patients and it is important they empathise it then they can recognise problems when they arise.
The pare and its appendages (nails, hair and certain glands) form the largest organ in the human torso, with a surface expanse of 2m2 (Hughes, 2001). The skin comprises 15% of the total developed body weight; its thickness ranges from <0.1mm at its thinnest role (eyelids) to 1.5mm at its thickest office (palms of the easily and soles of the feet) (Kolarsick et al, 2011). This article reviews its structure and functions.
Structure of the pare
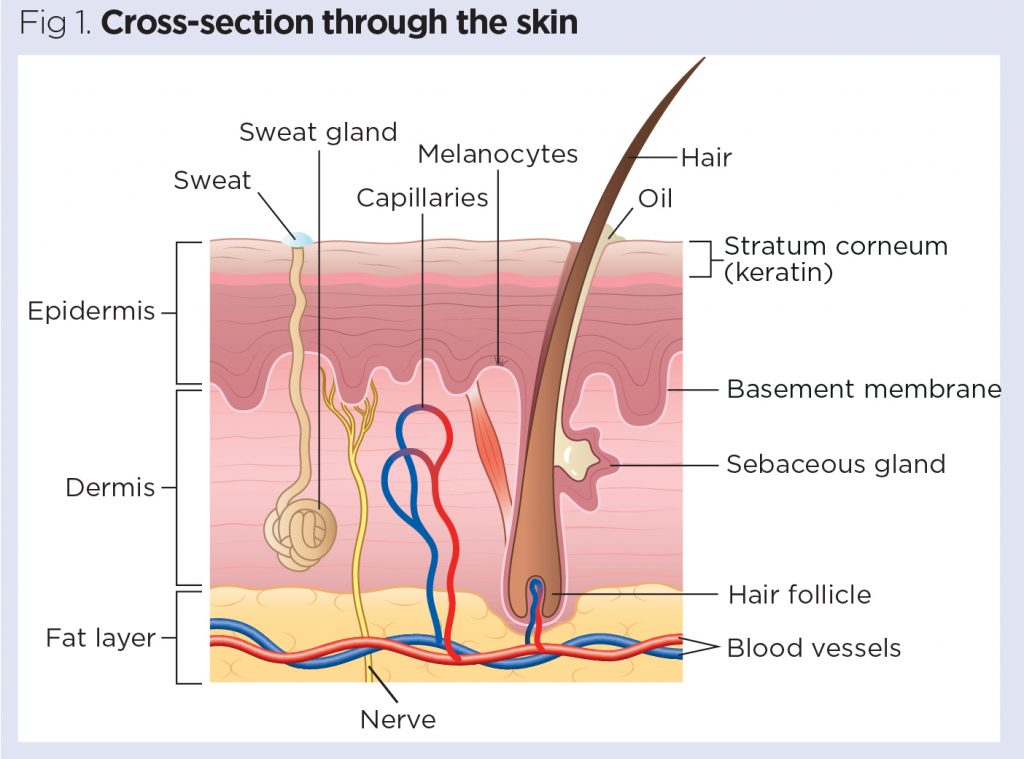
The skin is divided into several layers, as shown in Fig 1. The epidermis is composed mainly of keratinocytes. Below the epidermis is the basement membrane (also known equally the dermo-epidermal junction); this narrow, multilayered structure anchors the epidermis to the dermis. The layer below the dermis, the hypodermis, consists largely of fat. These structures are described below.
Epidermis
The epidermis is the outer layer of the peel, divers as a stratified squamous epithelium, primarily comprising keratinocytes in progressive stages of differentiation (Amirlak and Shahabi, 2017). Keratinocytes produce the protein keratin and are the major building blocks (cells) of the epidermis. As the epidermis is avascular (contains no blood vessels), it is entirely dependent on the underlying dermis for nutrient delivery and waste disposal through the basement membrane.
The prime office of the epidermis is to deed as a physical and biological barrier to the external environment, preventing penetration past irritants and allergens. At the same fourth dimension, it prevents the loss of water and maintains internal homeostasis (Gawkrodger, 2007; Cork, 1997). The epidermis is composed of layers; most torso parts take four layers, but those with the thickest skin have five. The layers are:
- Stratum corneum (horny layer);
- Stratum lucidum (only found in thick peel – that is, the palms of the hands, the soles of the anxiety and the digits);
- Stratum granulosum (granular layer);
- Stratum spinosum (prickle cell layer);
- Stratum basale (germinative layer).

The epidermis also contains other prison cell structures. Keratinocytes brand upward effectually 95% of the epidermal jail cell population – the others being melanocytes, Langerhans cells and Merkel cells (White and Butcher, 2005).
Keratinocytes. Keratinocytes are formed by division in the stratum basale. Every bit they motility up through the stratum spinosum and stratum granulosum, they differentiate to form a rigid internal construction of keratin, microfilaments and microtubules (keratinisation). The outer layer of the epidermis, the stratum corneum, is composed of layers of flattened dead cells (corneocytes) that take lost their nucleus. These cells are then shed from the skin (desquamation); this complete process takes approximately 28 days (Fig 3).

Between these corneocytes there is a complex mixture of lipids and proteins (Cork, 1997); these intercellular lipids are broken downwardly by enzymes from keratinocytes to produce a lipid mixture of ceramides (phospholipids), fatty acids and cholesterol. These molecules are arranged in a highly organised fashion, fusing with each other and the corneocytes to form the peel's lipid barrier against water loss and penetration past allergens and irritants (Holden et al, 2002).
The stratum corneum can exist visualised as a brick wall, with the corneocytes forming the bricks and lamellar lipids forming the mortar. As corneocytes contain a h2o-retaining substance – a natural moisturising factor – they attract and concord h2o. The high water content of the corneocytes causes them to bang-up, keeping the stratum corneum pliable and rubberband, and preventing the germination of fissures and cracks (Holden et al, 2002; Cork, 1997). This is an of import consideration when applying topical medications to the skin. These are absorbed through the epidermal barrier into the underlying tissues and structures (percutaneous absorption) and transferred to the systemic circulation.
The stratum corneum regulates the amount and charge per unit of percutaneous absorption (Rudy and Parham-Vetter, 2003). One of the almost important factors affecting this is skin hydration and environmental humidity. In salubrious pare with normal hydration, medication can merely penetrate the stratum corneum by passing through the tight, relatively dry, lipid barrier between cells. When peel hydration is increased or the normal skin barrier is dumb as a result of skin affliction, excoriations, erosions, fissuring or prematurity, percutaneous absorption will be increased (Rudy and Parham-Vetter, 2003).
Melanocytes. Melanocytes are institute in the stratum basale and are scattered among the keratinocytes along the basement membrane at a ratio of one melanocyte to 10 basal cells. They produce the pigment melanin, manufactured from tyrosine, which is an amino acrid, packaged into cellular vesicles called melanosomes, and transported and delivered into the cytoplasm of the keratinocytes (Graham-Chocolate-brown and Bourke, 2006). The main function of melanin is to blot ultraviolet (UV) radiation to protect usa from its harmful effects.
Skin colour is determined not by the number of melanocytes, merely by the number and size of the melanosomes (Gawkrodger, 2007). It is influenced past several pigments, including melanin, carotene and haemoglobin. Melanin is transferred into the keratinocytes via a melanosome; the colour of the pare therefore depends of the amount of melanin produced past melanocytes in the stratum basale and taken upward by keratinocytes.
Melanin occurs in 2 primary forms:
- Eumelanin – exists equally black and brown;
- Pheomelanin – provides a cherry colour.
Pare colour is also influenced by exposure to UV radiations, genetic factors and hormonal influences (Biga et al, 2019).
Langerhans cells. These are antigen (micro-organisms and strange proteins)-presenting cells found in the stratum spinosum. They are part of the torso's immune system and are constantly on the sentry for antigens in their surroundings so they can trap them and present them to T-helper lymphocytes, thereby activating an allowed response (Graham-Chocolate-brown and Bourke, 2006; White and Butcher, 2005).
Merkel cells. These cells are simply present in very small numbers in the stratum basale. They are closely associated with terminal filaments of cutaneous nerves and seem to have a function in sensation, specially in areas of the body such as palms, soles and genitalia (Gawkrodger, 2007; White and Butcher, 2005).
Basement membrane zone
(dermo-epidermal junction)
This is a narrow, undulating, multi-layered structure lying between the epidermis and dermis, which supplies cohesion between the two layers (Amirlak and Shahabi, 2017; Graham-Brown and Bourke, 2006). It is composed of two layers:
- Lamina lucida;
- Lamina densa.
The lamina lucida is the thinner layer and lies direct beneath the stratum basale. The thicker lamina densa is in direct contact with the underlying dermis. It undulates between the dermis and epidermis and is connected via rete ridges called dermal papillas, which contain capillary loops supplying the epidermis with nutrients and oxygen.
This highly irregular junction profoundly increases the expanse over which the exchange of oxygen, nutrients and waste product products occurs between the dermis and the epidermis (Amirlak and Shahabi, 2017).
Dermis
The dermis forms the inner layer of the pare and is much thicker than the epidermis (1-5mm) (White and Butcher, 2005). Situated between the basement membrane zone and the subcutaneous layer, the primary role of the dermis is to sustain and support the epidermis. The main functions of the dermis are:
- Protection;
- Cushioning the deeper structures from mechanical injury;
- Providing nourishment to the epidermis;
- Playing an important role in wound healing.
The network of interlacing connective tissue, which is its major component, is made upwards of collagen, in the chief, with some elastin. Scattered within the dermis are several specialised cells (mast cells and fibroblasts) and structures (claret vessels, lymphatics, sweat glands and nerves).
The epidermal appendages also lie inside the dermis or subcutaneous layers, just connect with the surface of the skin (Graham-Brown and Bourke, 2006).
Layers of dermis. The dermis is made upwards of ii layers:
- The more superficial papillary dermis;
- The deeper reticular dermis.
The papillary dermis is the thinner layer, consisting of loose connective tissue containing capillaries, elastic fibres and some collagen. The reticular dermis consists of a thicker layer of dense connective tissue containing larger blood vessels, closely interlaced elastic fibres and thicker bundles of collagen (White and Butcher, 2005). Information technology also contains fibroblasts, mast cells, nerve endings, lymphatics and epidermal appendages. Surrounding these structures is a mucilaginous gel that:
- Allows nutrients, hormones and waste material products to pass through the dermis;
- Provides lubrication between the collagen and rubberband fibre networks;
- Gives majority, assuasive the dermis to act as a shock absorber (Hunter et al, 2003).
Specialised dermal cells and structures. The fibroblast is the major cell type of the dermis and its main office is to synthesise collagen, elastin and the mucilaginous gel within the dermis. Collagen – which gives the skin its toughness and strength – makes upwardly 70% of the dermis and is continually cleaved downwardly and replaced; elastin fibres requite the peel its elasticity (Gawkrodger, 2007). Even so both are affected by increasing age and exposure to UV radiations, which results in sagging and stretching of the skin equally the person gets older and/or is exposed to greater amounts of UV radiation (White and Butcher, 2005).
Mast cells incorporate granules of vasoactive chemicals (the principal one being histamine). They are involved in moderating immune and inflammatory responses in the skin (Graham-Dark-brown and Bourke, 2006).
Blood vessels in the dermis form a complex network and play an important part in thermoregulation. These vessels can be divided into ii distinct networks:
- Superficial plexus – made up of interconnecting arterioles and venules lying close to the epidermal border, and wrapping around the structures of the dermis, the superficial plexus supplies oxygen and nutrients to the cells;
- Deep plexus – found deeper at the border with the subcutaneous layer, its vessels are more substantial than those in the superficial plexus and connect vertically to the superficial plexus (White and Butcher, 2005).
The lymphatic drainage of the skin is important, the main office existence to conserve plasma proteins and scavenge strange cloth, antigenic substances and bacteria (Amirlak and Shahabi, 2017).
About one million nerve fibres serve the skin – sensory perception serves a critically important protective and social/sexual function. Costless sensory nerve endings are found in the dermis as well as the epidermis (Merkel cells) and find pain, itch and temperature. In that location are as well specialised receptors – Pacinian corpuscles – that detect pressure and vibration; and Meissner's corpuscles, which are touch-sensitive.
The autonomic nerves supply the blood vessels and sweat glands and arrector pili muscles (fastened to the hair) (Gawkrodger, 2007).
Hypodermis
The hypodermis is the subcutaneous layer lying beneath the dermis; information technology consists largely of fat. It provides the master structural support for the skin, as well as insulating the body from cold and aiding daze absorption. Information technology is interlaced with blood vessels and fretfulness.
Functions of the peel
The skin has three main functions:
- Protection;
- Thermoregulation;
- Sensation.
Inside this, it performs several of import and vital physiological functions, as outlined below (Graham-Brown and Bourke, 2006).
Protection
The skin acts as a protective barrier from:
- Mechanical, thermal and other physical injury;
- Harmful agents;
- Excessive loss of wet and poly peptide;
- Harmful effects of UV radiation.
Thermoregulation
1 of the skin's important functions is to protect the body from cold or heat, and maintain a constant core temperature. This is achieved past alterations to the blood menstruum through the cutaneous vascular bed. During warm periods, the vessels dilate, the skin reddens and beads of sweat form on the surface (vasodilatation = more blood catamenia = greater direct estrus loss). In cold periods, the blood vessels constrict, preventing heat from escaping (vasoconstriction = less blood menstruation = reduced rut loss). The secretion and evaporation of sweat from the surface of the skin also helps to cool the body.
Sensation
Pare is the 'sense-of-touch' organ that triggers a response if nosotros touch on or experience something, including things that may cause pain. This is important for patients with a pare status, as pain and itching tin can exist extreme for many and cause keen distress. Also touch is important for many patients who experience isolated by their pare as a result of colour, affliction or the perceptions of others as many experience the fact that they are seen equally dirty or contagious and should not exist touched.
Immunological surveillance
The skin is an of import immunological organ, fabricated up of cardinal structures and cells. Depending on the immunological response, a diverseness of cells and chemic messengers (cytokines) are involved. These specialised cells and their functions will exist covered afterward.
Biochemical functions
The pare is involved in several biochemical processes. In the presence of sunlight, a form of vitamin D called cholecalciferol is synthesised from a derivative of the steroid cholesterol in the peel. The liver converts cholecalciferol to calcidiol, which is then converted to calcitriol (the active chemical form of the vitamin) in the kidneys. Vitamin D is essential for the normal absorption of calcium and phosphorous, which are required for healthy bones (Biga et al, 2019). The skin too contains receptors for other steroid hormones (oestrogens, progestogens and glucocorticoids) and for vitamin A.
Social and sexual function
How an individual is perceived by others is important. People make judgements based on what they see and may form their first impression of someone based on how that person looks. Throughout history, people take been judged considering of their skin, for example, due to its colour or the presence of a peel condition or scarring. Skin conditions are visible – in this peel-, beauty- and image-conscious guild, the fashion patients are accustomed by other people is an important consideration for nurses.
Summary
This article gives an overview of the construction and functions of the skin. Role 2 will provide an overview of the accessory structures of the skin and their functions.
Key points
- The skin is the largest organ in the human trunk
- Approximately half of the UK population will experience a skin condition in any given yr
- Nurses observe patients' skin daily, so need to be able to identify problems when they arise
- Cardinal functions of the skin include protection, regulation of body temperature, and sensation
- How others respond to people who accept pare conditions is an of import consideration for nurses

- Examination your knowledge with Nursing Times Self-assessment later on reading this article. If you score eighty% or more, you will receive a personalised certificate that you tin can download and shop in your NT Portfolio as CPD or revalidation evidence.
- Have the Nursing Times Cocky-assessment for this article
References
All Parliamentary Group on Peel (1997) An Investigation into the Adequacy of Service Provision and Treatments for Patients with Skin Diseases in the UK.
Amirlak B, Shahabi L (2017) Pare Anatomy.
Biga LM et al (2019) Anatomy and Physiology.The integumentary organisation 5.i: layers of the skin.
Cork MJ (1997) The importance of pare barrier function. Journal of Dermatological Treatment; 8: Suppl 1, S7-S13.
Gawkrodger DJ (2007) Dermatology: An Illustrated Color Text. Edinburgh: Churchill Livingstone.
Graham-Brown R, Bourke J (2006) Mosby'south Color Atlas and Text of Dermatology. London: Mosby.
Holden C et al (2002) Brash best practice for the use of emollients in eczema and other dry skin conditions. Periodical of Dermatological Treatment; 13: 3, 103-106.
Hughes Due east (2001) Peel: its structure, role and related pathology. In: Hughes E, Van Onselen J (eds) Dermatology Nursing: A Applied Guide. Edinburgh: Churchill Livingstone.
Hunter J et al (2003) Clinical Dermatology. Oxford: Blackwell Scientific discipline.
Kolarsick PAJ et al (2011) Anatomy and physiology of the skin. Journal of Dermatology Nurses' Association; iii: 4, 203-213.
Rudy SJ, Parham-Vetter PC (2003) Percutaneous absorption of topically applied medication. Dermatology Nursing; 15: ii, 145-152.
Schofield J et al (2009) Skin Conditions in the UK: A Health Care Needs Cess.
White R, Butcher M (2005) The structure and functions of the skin. In: White R (ed) Peel Care in Wound Management: Assessment, Prevention and Treatment. Aberdeen: Wounds Uk.
Source: https://www.nursingtimes.net/clinical-archive/dermatology/skin-1-the-structure-and-functions-of-the-skin-25-11-2019/
Posted by: currietintery.blogspot.com
0 Response to "What Is The Composition Of Our Skin"
Post a Comment